Save The Date: Reception and Annual Fundraiser
Join us at the College Football Hall of Fame on December 4, 2014
to celebrate the life and legacy of the late Jack Kemp.
Join us at the College Football Hall of Fame on December 4, 2014
to celebrate the life and legacy of the late Jack Kemp.
Junior Achievement (JA) of Georgia has created an interactive, marketplace environment where children’s dreams about future careers actually come to life. Set in the fictitious community of JA BizTown, students have the opportunity to experience a day-in-the-life of a working professional.
A Microcosm of Atlanta
Located in the Georgia World Congress Center, BizTown is an interactive community that serves as a microcosm of the Atlanta business community. Representing such businesses as Chick-Fil-A, AT&T, UPS, Bank of America, Wells Fargo, Delta, RockTenn Recycling, and the Atlanta Falcons, the space is masterfully designed with authentic store fronts, a central, artificial lawn, and a stage for the mayor and CEOs to give town speeches. The realistic design of the space and the energy of the students make the town feel like it has come to life.

Interactive Learning Environment
The purpose of BizTown is to create a learning environment where students have the opportunity to experience what it is like to be an employee, tax-payer, and consumer. Within their respective companies, students are given the responsibility of carrying out their job assignments for such positions as CEO, CFO, sales manager, and marketing director. They are expected to quickly learn these job responsibilities, become acclimated to their unique business environment, and contribute to the day-to-day operations of their company, effectively simulating a “first-day-on-the-job” experience.
However, students’ experience at BizTown is not the only time where they have had a chance to discuss what it is like being a part of the global economy. In fact, prior to arriving in this community, students complete three weeks of JA-provided coursework which interweaves concepts of practical economics, career awareness, and entrepreneurship.
Their time in BizTown serves as a culmination of their learning experience where they have a chance to put into practice what they have learned in a fun and interactive way.
In addition to teaching students to balance the demands of job assignments, this hands-on model makes learning basic financial literacy concepts fun. Within the span of four hours, students learn how to develop a personal budget, deposit a paycheck at the bank, and make purchasing decisions. Many of the middle school students for which BizTown is geared have likely never written a check or balanced a checkbook before participating in this program. Participating in this simulation gives them the chance to practice these skills among their classmates and see how they are necessary for becoming a responsible consumer.
Bridging the Business and Education Community
Business and community volunteers play a key role in making BizTown a success. They are responsible for overseeing the students in each of the businesses, ensuring that they know their work responsibilities and are able to carry them out.
While the students work, volunteers are able to share practical tips and life lessons which serve to make the learning experience even more powerful.
This interaction gives the volunteers a chance to give back to their community by preparing the next generation for both professional and personal success.
Personal Reflections
Several Georgia Center for Opportunity (GCO) team members recently had the privilege of spending a day volunteering at BizTown. Here’s what a few of them wrote in reflecting about their experience:
Aundrea Gregg – “I was not only impressed with the overall setup of Junior Achievement’s Biz Town, I was also blown away by the hard work and business sense of the students I had the pleasure of working with on my volunteer day. As I helped out at the Delta shop, it was endearing to watch students develop pricing and marketing strategies, practice customer service skills, and for the students who acted as the CEO and CFO, get a taste of managing employees and running a company.
Chris Elder – “The immersiveness of the JA BizTown environment combined with the fast-paced tasks really kept the kids focused on the simulation. The students I helped thoroughly embraced their roles and often found themselves needing to prioritize and make tradeoffs in how they should spend their time.
“It was great exposure to some very important non-academic skills.”
Michael Schulte – “Overseeing the students assigned to RockTenn Recycling, I observed the challenges of running the day-to-day operations of a business. Not only can the accounting become a nightmare if you don’t stay on top of it, but making sure the employees are doing their tasks (and are equipped for their job) is a major challenge…This program wonderfully simulates a ‘real work’ experience.”
Katherine Greene – “I had the pleasure of coaching a group of sixth graders as they ran the operations of a Chick-Fil-A restaurant…In the real world, these students may not have been old enough to work, vote, or be the boss, but they were learning how to manage a restaurant, write checks, deposit checks, have staff meetings, pay bills, earn money, purchase goods, and even vote for a mayor. I commend JA Biztown for helping the students to experience the hustle and bustle of a real community.”
A Shared Vision
The investment that JA is making in students’ lives to prepare them for future success is commendable. Its strategy of involving local business and community volunteers to achieve this goal aligns well with the work GCO is doing within our Breakthrough Norcross Initiative. Both JA and GCO desire to see students dream big and reach their full potential, and we know that this is only possible as members in the community see it as their responsibility to help make this happen.
In addition, Aundrea Gregg found a common thread between the work she is doing with GCO and the work JA is doing with students at BizTown. Listen to her words as she describes the potential that this program has in continuing to shape future leaders in our state:
“After the first business period, one of the flight attendants said, ‘Is this what your day is like? Being an adult is so much work!’ By the second business period, however, everyone seemed to have found their groove and the same young lady said ‘Eh, it’s not so bad after all!’
“The ‘light bulb moments’ that I witnessed were exactly what made the day so special.”
“Thinking on my work for the College and Career Pathways initiative, it is also those light bulb moments that drive home the importance of bridging in-classroom learning with hands-on practice in real-life scenarios. I am excited for all the knowledge the students gained at BizTown, and that this program may soon reach many more students across the state.”
A BizTown program is slated to open up in Gwinnett sometime soon.
Image Credit: Atlanta Public Schools (featured image) and Junior Achievement of Georgia

Click this link to register for the event: secure.foropportunity.org/breakthroughshowcase

Every Georgian is affected by the criminal justice system in some way. Whether it is paying taxes to fund the more than a billion dollars spent on prisons each year or knowing a loved one who has spent time behind bars, the justice system is becoming an increasingly familiar issue in the lives of Georgians.
In 2009, the Pew Center on the States released a report revealing that 1 in 13 adults were under some form of correctional supervision in Georgia. This means that over half-a-million Georgians were either in jail, in prison, on parole, or on probation that year. This percentage far surpassed the national average, which was still an astonishing 1 in 31 adults under correctional supervision.
Even more staggering, 2.6 million people have a criminal record on file with the Georgia Crime Information Center, while the state’s total population is 10 million people. The collateral consequences associated with having a criminal record mean that as many as 1 in 4 Georgians likely face barriers to obtaining employment, housing, and even voting.
Currently, 53,000 people are incarcerated in Georgia, giving the state the fifth highest prison population in the nation. The incarcerated population more than doubled between 1990 and 2011, while the state’s general population increased by only half that rate during the same time period.

The Merry-Go-Round
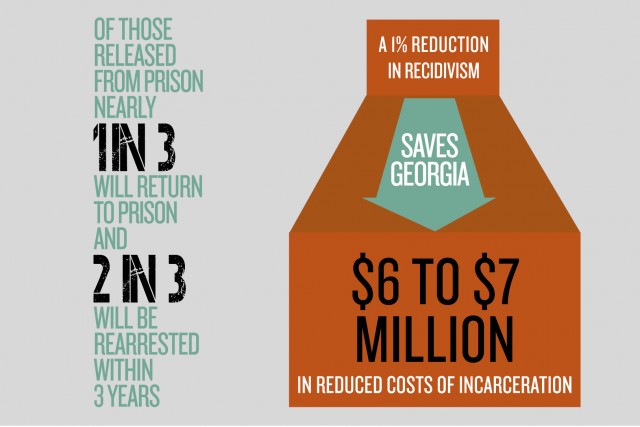
Once a person enters the system, his or her likelihood of staying in it is fairly strong. The state releases 20,000 prisoners back into the community every year, and 2 out of 3 of those released are rearrested within three years. Nearly 1 in 3 are re-convicted within this time frame, resulting in re-incarceration.
While the state reports a recidivism rate of 30 percent over the past decade (determined by the number of offenders who are reconvicted within three years of release), the actual recidivism rate is closer to 50 percent – taking into account the number of people who commit a technical violation while on probation and parole, as well as the number of offenders who recidivate after the standard three-year time period.
The Cost
The effect of recidivism is very costly to the state: It negatively impacts public safety, results in burgeoning costs to taxpayers, and contributes to the breakdown of families.
Public Safety
Released offenders who continue to have unaddressed criminogenic (crime-producing) needs are likely to re-engage in criminal behavior and place themselves, their families, and their community at risk. Criminal behavior may arise from a substance abuse or mental health issue, from negative peer associations, from a poor family environment, from desperation caused by their inability to meet their basic needs for housing, employment, and transportation, and from a variety of other risk factors. Without addressing the underlying factors that lead returning citizens to engage in criminal behavior, the recidivism rate will continue to remain high as new crimes and technical violations of probation and parole are committed.
Taxpayers
Recidivism places a heavy burden on taxpayers. The cost to incarcerate one person for a year in Georgia is $21,000 – more than twice the amount the state spends toward educating one student for a year. This means that every cohort of released prisoners that recidivates amounts to $130 million annually, given the 30 percent recidivism rate and the 20,000 offenders released each year. Further, state expenditures on incarceration reached $1.1 billion in fiscal year 2010 – more than twice the amount spent in 1990, which was $492 million. For the amount taxpayers have spent on the prison system in recent years, the outcomes have been unacceptable.
Families
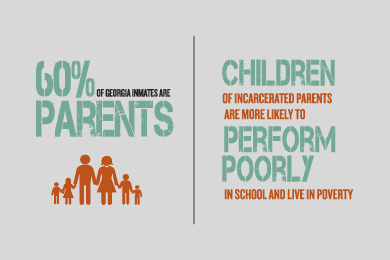
Finally, a person cycling in and out of prison creates instability in the life of his or her family. Significantly, 60 percent of inmates in Georgia are parents, and a number of these parents have been incarcerated more than once. Children of incarcerated parents are more likely to perform poorly in school, to be exposed to their parent’s substance abuse, to use drugs, to experience mental health issues, to experience domestic violence, and to live in poverty. Incarceration puts a tremendous strain on existing relationships, decreases the chances that partners will marry, transforms family roles, and often leads custodial parents to depend on public assistance. Families experience shame, anger, hurt, and despair at the incarceration of loved ones, creating inner turmoil that is often never addressed.
What Can Be Done?
Because of the enormous costs posed by incarceration and recidivism, it is essential for Georgia to promote solutions that will address underlying issues returning citizens face. This effort must take place at all points along the continuum, from the Governor’s Office down to individuals in the community.
Several areas of reform that Georgia Center for Opportunity’s Prisoner Reentry Working Group has addressed to improve reentry outcomes involve increasing employment opportunities (read report), restructuring debt, and developing the criminal justice and service provider workforce.
Employment
Employment plays a critical role in reducing offender recidivism, as it has the power to deter ex-offenders from crime and incentivize law-abiding behavior. Key barriers to employment that the working group identified include driver’s license suspensions, missing identification (i.e., Social Security cards and birth certificates), professional license restrictions, and employers’ negative perceptions.
To remove these barriers, the group recommended that the state lift suspensions on driver’s licenses for people who committed a non-driving related drug offense, offer incentives to employers to hire those with a criminal record, and have public and private employers postpone the question about an applicant’s criminal history to a later point in the interview process. Several of these recommendations were signed into law in April 2014.

Debt
Various state agencies enforcing the payment of debts and obligations without considering the needs and financial circumstance of returning citizens can lead them to recidivate. Returning citizens often carry excessive debt because of missed child support payments that accrue during their incarceration, court-imposed fees, fines, and surcharges for their offense, unpaid restitution, and the inability for them to earn money while in prison.
Several steps that the state can take to encourage returning citizens to repay this debt in a realistic manner include: Identifying offenders with child support orders upon entry to prison; providing offenders with pertinent information about their child support responsibilities; providing a grace period of 90 days upon release that gives returning citizens the opportunity to find a job and get back on their feet; and providing incentives for returning citizens to pay current obligations of child support and restitution by forgiving a portion of fines, fees, surcharges, and child support arrears owed to the state.
Workforce Development
There is an urgent need for the criminal justice workforce and community service providers to be trained in delivering evidence-based programs and practices. Without proper training and implementation, Georgia’s recidivism rate is likely to remain unchanged.
The state can better ensure successful reentry outcomes are reached by providing training and support to agencies and service professionals in the use of evidence-based practices, developing a hybrid degree program that combines criminal justice training and case management techniques, ensuring a risk/needs assessment is used and followed from entry into prison to treatment in the community, providing the workforce the ability to use graduated sanctions and incentives, and providing accountability to the workforce to ensure evidence-based practices are being used.
Conclusion
Each person involved with this reentry effort, from the governor to mentors in the community, need to put into practice what has shown to work in reducing recidivism. This effort will require education, training, resources, and coordination on all fronts, and it is one that should be pursued with fidelity. Doing so will help to bring restoration to families, build stronger communities, and ensure a more just society.

Click here to view The State of Corrections infographic

Image retrieved from iamgifted.org.
Georgia Center for Opportunity (GCO) desires to see students flourish. As a way of realizing this vision, GCO supports organizations that have a similar heartbeat to see students succeed. One such organization is the Gifted Education Foundation (Gifted).
This summer, GCO had the privilege of hosting Gifted’s founder, Anthony Flynn, for a Lunch & Learn where he discussed how Gifted got started and the impact it is making in the community. Local high school students, education leaders, and various non-profit workers came to the event to learn more about this promising organization.
Flynn opened the session by sharing an inspiring testimony about his life.
Born to a 17-year-old single mother in Memphis, Tennessee, his childhood was marked by upheaval and transition. Nonetheless, he overcame adversity and earned a scholarship to play football at Tennessee Tech University. College proved to be another period of trials, however, as he found himself surrounded by peers who made negative choices. After attending this school for just a semester, he decided to transfer to the University of Memphis where he would go on to graduate in four years.
After graduating from college, Flynn continued his education and earned a Master of Arts (Religion) from Memphis Theological Seminary. During this time, he worked as a student pastor where he served and mentored many at-risk students. This work led him to become involved in sustainable urban development that focused on restoring the economic, educational, and social foundation of his community, and later to serve as president of a national organization that trains urban leaders to impact America’s 250 most at-risk zip codes. From these experiences, Flynn went on to found Gifted in 2012.
Gifted exists to produce first generation college graduates and marketplace leaders from low-income communities across America. It is built upon the premise that every child has the potential to succeed if given the opportunity and guidance he or she needs.

Image retrieved from iamgifted.org.
Flynn believes that although “16 million American children are growing up in poverty,” they do not have to stay there. They can move forward “with the right educational opportunities and a structured system of leaders guiding them through a proven process.”
Providing this opportunity and guidance is precisely what Gifted seeks to do.
As a way of accomplishing this mission, Gifted has developed a four-phased strategy. Each phase prepares students for their next step in life, equipping them with the skills and resources needed to maximize their potential:
Phase 1: The Gifted Preparatory School
The first phase of the strategy involves preparing high school students for college, careers, and the rest of their life by teaching them general life skills, improving their ability to take standardized tests, building college and career awareness, and directing students toward scholarship and financial aid options.
Phase 2: The Gifted College Access Program
The second phase is designed to serve a select group of students who receive comprehensive life skills development and college readiness training. This training occurs on a college campus throughout students’ junior and senior years of high school. The focus is on improving their writing and standardized test-taking abilities, guiding them through the college application process, scholarships and financial aid, and strengthening their life skills in the realm of decision-making, conflict resolution, and time management, among others.
Phase 3: The Gifted Mentoring Program
The third phase provides students who successfully complete the Gifted College Access Program with hands-on, experiential coaching through the Gifted Enrichment and Retention Curriculum. Each student is assigned to a Life Development Coordinator and placed in cohorts where life-on-life accountability and support is deliberated throughout their entire undergraduate education. Students will also participate in leadership development programs, internships, fellowships, and research graduate school options.
Phase 4: The Gifted Leadership Program
Finally, the fourth phase consists of two tiers:
The first tier will provide college graduates with a key marketplace partner who will serve as a life and career mentor. Graduates will work to develop short, medium, and long-term goals in a variety of life categories. In addition, they will cultivate leadership skills, work to enhance existing relationships, and develop a civic and community engagement plan.
The second tier is for graduates who have the criteria in place to become marketplace leaders. They will receive preparation for mid-level to senior-level executive leadership roles in the marketplace, mentor at least one student in the Gifted program, receive training and opportunity for philanthropy and high-impact community involvement, and be trained to serve as entry-level board members for community and non-profit organizations.

Image retrieved from http://iamgifted.org.
Through the implementation of this strategy, Gifted hopes to achieve three outcomes over the course of a student’s involvement with the program. The first is that Gifted students graduate high school equipped with academic and life skills necessary to enroll in and be successful at a four-year college/university. The second is that Gifted students graduate college and are successfully hired in the marketplace or enrolled in graduate school within six months of college graduation. The third is that Gifted alumni take on the responsibility of mentoring at least one other student within six months of their graduation.
Cultivating the mentality of giving back is important for the continued success of the program and for growing lifelong, benevolent people that will continue to serve their communities.
Gifted’s comprehensive approach prepares students to be successful in college, in their career, and in life. For this reason, GCO is proud to encourage community partners to support Gifted in seeing students reach their full potential.
To learn more about Gifted, get involved with their work, or read stories about their success, visit http://iamgifted.org/.